


A Community Based Rehabilitation (CBR) worker video capturing physical status of a disabled child.
Jan Vikas Samiti established the Tele-Rehabilitation initiative “Sambhav” to reach out to children with neurological disabilities in resource poor settings. The project’s objective is to tailor rehabilitation plans and provide appropriate therapy to children with impairments, as well as increase field workers’ competence for diagnosis and the development of suitable rehabilitation plans. Tele-rehabilitation is a clinical term that refers to the delivery of consultative, preventive, diagnostic, and therapeutic rehabilitation treatments using two-way interactive tele communications technology.
It is designed to provide reasonable access to geographically remote people and to those who are physically and financially impoverished. Tele-Rehabilitation can also be used to improve the nature of rehabilitation medical care administrations. This cutting-edge recuperation technique interfaces with the administrations given by a few health care specialties, for example, physiotherapy, discourse pathology, language-related treatment, and biomedical design. It enhances the situation, strength, and duration of therapy, which is typically impracticable within the constraints of conventional health care frameworks.
The primary objective and focus of the endeavor, Sambhav, is to utilise an internet interface and a mobile application to assess and recover plans, progress, and outcomes.
 Click here to have an Overview of the Tele-Rehab. Program
Click here to have an Overview of the Tele-Rehab. Program
Research Paper Final- IMPACT Telerehabilitation Project Sambhav
Telerehabilitation Evaluation Report
Need:
On the role of telemedicine in the health care service delivery, a patient survey predicts that 75% of all patients expect to use digital services in future. 75% of the country’s healthcare infrastructure is concentrated in urban areas while more than 75% of the population lives in rural areas. The majority (69%) of the persons with disabilities reside in rural areas. 71 % of children with disabilities live in rural India and facing a range of barriers. E- Rehabilitation technology will thus provide an opportunity to serve the poorer and marginalized sections of the community.
Benefits:
- Best benefit for the end-user (i.e., an individual with a disability) within their environment
- Therapist does not need to visit service user at their home
- Better clinical support in local communities
- Improved access to specialized services
- Caregivers/service users need not to overcome structural barriers when want to access the rehabilitation service
- Caregivers need not go to rehabilitation centre
- Decreased travel between rural communities and rehabilitation centre, cost-effective, and reduce the cost of rehabilitation (centre-based)
- Tele rehabilitation is equally as effective as conventional rehabilitation in improving activities of daily living, motor function, and quality of life
- Tele-rehabilitation now changing ways of thinking and acting in service delivery provision and hope to cover the maximum living in the remote terrains
Tele-rehabilitation in CBR setting:
- Tele-rehabilitation can be used to improve Community Based Rehabilitation (CBR) systems, particularly in developing countries where rehabilitation services are very expensive and not available at the community level. Community-based rehabilitation programs can be strengthened by using tele rehabilitation, and that tele-rehabilitation can address the underserved needs of persons with disabilities located in the remote area.
- Tele-rehabilitation can provide synchronous and comparatively low cost but quality rehabilitation services regardless of time, space, and location. It’s flexibility, remote availability, and cost-effectiveness is helpful for community-based settings.
- Tele-rehabilitation methodology can be used to provide rehabilitation services to achieve WHO goals (e.g., improved access to health care services and professionals).
- The use of digital technology in the CBR/CBID has extended the scopes of various professionals working in the field of rehabilitation to reach the maximum and found tele-rehabilitation is as effective as conventional rehabilitation.
Package: Tele-rehabilitation / (E-rehabilitation):
JVS is willing to offer tele-rehabilitation services to interested NGOs/Rehabilitation units/Hospitals to link and expand their services to wider areas with expert guidance and support for the diagnosis and plan in terms of physical rehabilitation of children with disabilities for very nominal charges with mutual agreement on a no-profit basis.
Continuation of existing partner organizations:
After the end of the contract on 31 December 2020, all existing POs in tele-rehabilitation project may give their consent to extend the contract which was made at the beginning of the project with JVS. For the extended contract, the existing POs will be able get case-based consultation services for a nominal fee on no-profit basis.
Understanding project “Sambhav”: (JVS Tele-rehabilitation Unit):
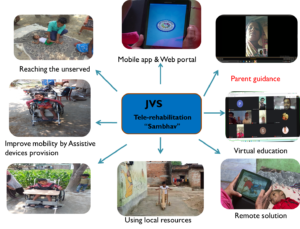
With the rapid evolution of digital technology seen as an opportunity to improve rehabilitation services in remote parts of the country, Jan Vikas Samiti has introduced tele-rehabilitation project “Sambhav” with a motto reaching the unreached using the web portal and the mobile app for better individual rehabilitation plan and service delivery. The project “Sambhav” aims to capacitate CBR facilitators on rehabilitation diagnosis, making custom made treatment/rehabilitation plans and providing appropriate therapies to the children and youth with disabilities who are most in need in the rural parts of India using recent technology. The main purpose and focus of the project Sambhav is the application of the web portal and mobile app for purpose of assessment and rehabilitation plan, progress and outcomes.
Methodology:
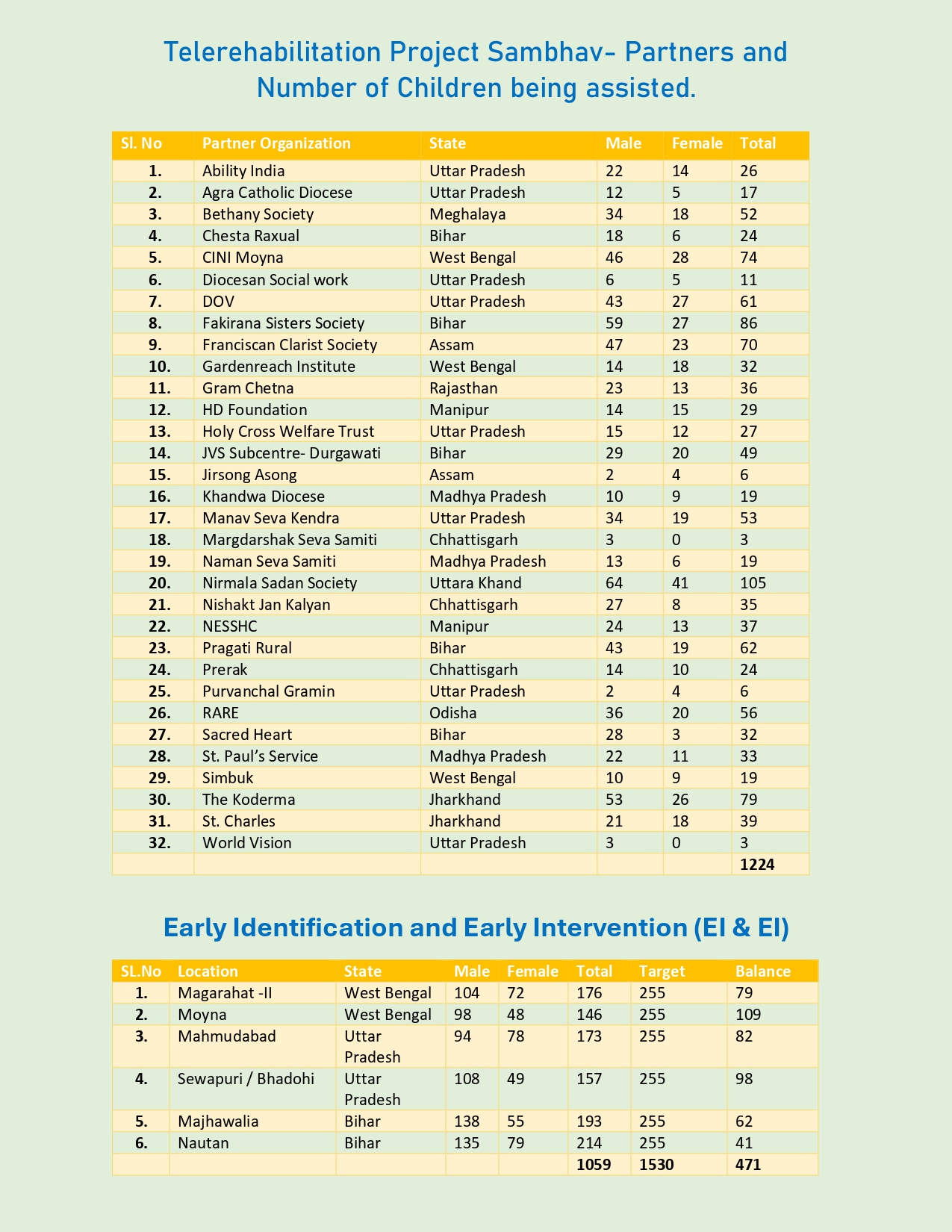
At present, JVS Tele-rehabilitation unit (ICT) is providing guidance for the physical rehabilitation service to selected Partner Organizations (POs) in Uttar Pradesh, Bihar, Uttarakhand, Jharkhand and Madhya Pradesh under this project. A protocol for the physical rehabilitation diagnosis/planning of children with developmental disabilities is made at JVS to help the selected partner organizations to develop their capacities in term of providing quality physical rehabilitation service. To provide better Tele-rehabilitation service delivery, regular training programs are conducted for selected CBR workers from the Partner Organisations (POs) on video filming and the use of rehabilitation protocol. Web portal and Mobile app on Tele-rehabilitation is developed by JVS and the same is shared with the selected CBR workers. Store and Forward (in which after video shooting, it can be stored and at the time of need can be forwarded to the JVS headquarter for intervention planning) method of technology which is quite practical and suites well to the concept of tele-rehabilitation and as per need real-time interaction and guidance have been provided to the parents/caregivers and field staffs as well. Rehabilitation professional/expert at JVS Tele-rehabilitation unit regularly receives videos of children with disabilities and assesses the case and provides treatment protocol/rehabilitation plan to the POs and periodically monitors the progress of cases.
Outcomes:
Tele-rehabilitation service delivery will give the best benefit to the end-user (i.e., an individual with a disability) within their environment. It optimizes the timing, intensity and duration of therapy that is often not possible within the constraints of face-to-face treatment protocols in current health systems. From the inception of the program in mid-2018 to May 2020 more than 350 children with disabilities are assessed and their rehabilitation plan have been made in the pilot phase. PO heads and field staff have shared that they are now able to provide quality intervention in remote areas as per the physical rehabilitation protocol through tele-rehabilitation.
Current Partners

“Believe you can and you’re halfway there”
 Dilraj 5-year-old is a child with Cerebral Palsy Diplegia. He is the only child of his parents. His father is a teacher, in a government school. And his mother is a housewife. They are not sufficiently economically well; still they look after the child well, giving time for the child, for his exercises, physiotherapy etc.
Dilraj 5-year-old is a child with Cerebral Palsy Diplegia. He is the only child of his parents. His father is a teacher, in a government school. And his mother is a housewife. They are not sufficiently economically well; still they look after the child well, giving time for the child, for his exercises, physiotherapy etc.
The parents tried to treat him from his child hood onwards, as they found him very sick and he was not able to cope up with the normal growth of any child and they look him to a few doctors in Koderma and outside for his treatment, , but somehow he was not making any improvement .
He could not keep his both legs parallel down on the floor , it used to be up always, and so he was unable to stand or walk properly, not even with the support and help of others, and because of that he was not able to stand not even with a support. His back was very weak, it used to be very loose, where he could not keep himself straight. He was unable to speak. He is intellectually average, and is able to understand everything and respond to it easily.
It was very difficult to convince the parents in order to enroll him with Sambhav-Tele-Rehabilitation Program, because they were very disappointed with the physical condition of the child. As our KFCS team and especially because of the various and many efforts of our CBR staff, their constant visit , guidance to the child and parents, many counselling sessions, the parents began to give him more time, and attention and the child began to improve himself.
Now, Dilraj is trying to keep his legs down and there is a lot of improvement on his both legs. And since he is able to keep the both legs down, and with the support he is able to stand up now, and since he began to stand up and make movement of the body, his back bones is slowly becoming better, and strong. And since he began to come out of his house, he has become freer with others, and began to speak something, where he was never used to speak with anyone earlier. The tightness of his body is much better and it seems slowly improving. And as he began to speak and he began to learn something, and now he has completed studying Hindi and English letters orally, and we insist on the parents to start teaching him to write the letters and alphabets, and he has started slowly.
We wish that he will improve himself, and we are very thankful to all the staff of JVS-LF for this great work, encouragement, timely training and equipping our CBR staff.
“Disability cannot stop me from becoming a complete personality”
 Abhijit Kumar is a child with CP quadriplegia. He is from very poor family and his parents are illiterate. His father is a daily laborer and mother is a housewife. He has one elder brother of 18 years old and a younger sister 2 years old, both of them are in good and healthy condition. His family is economically very poor, even though they have a small portion of land and so on.
Abhijit Kumar is a child with CP quadriplegia. He is from very poor family and his parents are illiterate. His father is a daily laborer and mother is a housewife. He has one elder brother of 18 years old and a younger sister 2 years old, both of them are in good and healthy condition. His family is economically very poor, even though they have a small portion of land and so on.
Abhijit is a child with CP quadriplegia. He is a bed ridden child, always remained in bed. Even though he was treated in the beginning, but because of the ignorance and negligence of the parents and the family members, and also because of the lack of economical problems he could not bring any improvement on his physical condition. The child seemed always crying and never tried to crowl, or makes any movement. So he could not keep his neck, legs, hands etc. straight and steady. In this crucial physical condition, we joined this child with the JVS-Sambhav program and began to make frequent visit, counseling to the parents and timely guidance to the parents.
Our staff made various and many efforts through their frequent visit, guidance, counseling and providing the needed assistive devices and therapy, the child began to show improvement. As we noticed the child used to cry, whenever we make sit down and make him stand up, but slowly he stopped crying, by which we understood that there is no further difficulties the child is facing, as we make him sit down and stand with full support and help. As he began to sit, we found out that there is no control over the neck and head, there was saliva dropping etc. very badly. As the staff spent many days in doing therapy and frequent visit, there was improvement in controlling his neck and droppings by which the parents and the family members were surprised and encouraged and hoped that the child would improve. The child started to look here and there and it seemed that he is freed from some kind of blocks and bandages.
BY the constant effort of our staff and also of the parents, Abhijit who never touched any food by himself began to eat certain food, which he could hold like biscuits, etc and is trying to eat by himself, slowly. He also tries to drink water by himself. He started to hold the ball and other small playing items in his own hands. He also started to show expressions of hunger, toilet purpose, sleep etc. Even though he had AFO with him, they were never using it, but later on as they witnessed the improvement they started to use it and with this support he is able to stand for little time. In the initial stages the parents were not cooperating with us, because they could not see any improvement in the child whenever they had taken him for the treatment. But at present, they were very happy to see the improvement in the child, and started to cooperate with us in all that we suggest for the child and is readily began to give sufficient time for the therapy, other exercises etc. for the child and with the child.
We hope that this child can bring more improvement in the coming months.